









Is Uganda losing the fight against cervical cancer?
- Chris Tinka

- Jul 16, 2020
- 6 min read
Updated: Aug 22, 2020

Some parents in Uganda shun vaccinating their children against human papillomavirus because they fear that their daughter will become barren or face reproductive complications in adult life.
Cervical cancer is caused by the human papillomavirus (HPV), a common infection spread through close skin-to-skin contact, usually during sex or oral sex.
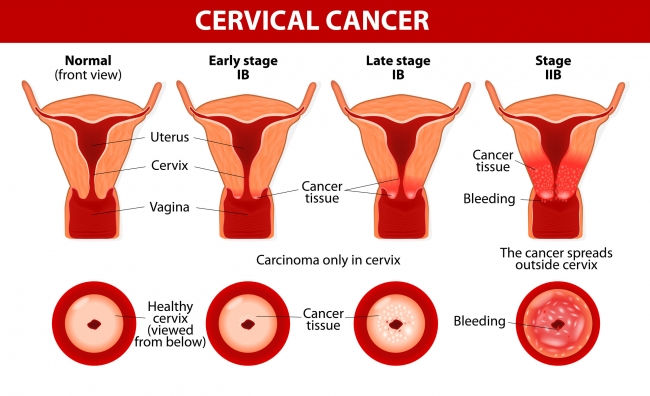
Dr Noleb Mugisha, an oncologist at the Uganda Cancer Institute, Mulago, defines cancer of the cervix as an abnormal and uncontrolled growth of cells in the cervix, resulting in wounds and bleeding.

The World Health Organisation (WHO) indicates that there are more than 200 types of human papillomavirus (HPV).
Type 16 and 18 account for 70 per cent of all cervical cancer cases worldwide. HPV also causes vaginal, vulva and anal cancers while HPV type 6 and 11 are responsible for genital warts.
Sexually active young girls and women, females with multiple sex partners, persons with other genital infections and weakened immune systems are more susceptible to HPV.
You are likely to get HPV without even knowing it because the virus often has no signs or symptoms Dr Annet Kisakye explained to journalists.
The symptoms of cancer of the cervix may sometimes appear when the disease has reached an advanced stage.
Signs of HPV my present with bleeding and pain during sexual intercourse; lower abdominal pain, inter-menstrual bleeding, heavy menstrual bleeding and vaginal discharge with a bad smell.
Dr Annet Kisakye the immunization focal person at the World Health Organisation (WHO) states that Uganda is among the five countries with the highest rates in Africa.
8 out of every 10 women at the Uganda Cancer Institute are suffering from cervical cancer. 6413 Ugandan women are diagnosed with CC annually, with 4301 deaths attributed to the disease.
In comparison, there are about 2,500 new cases of cervical cancer in England annually.
The national health system projects that a quarter of these cases could be prevented with the newer methods of testing and vaccinations.
In neighbouring Rwanda, the incidence rate currently stands at about 42 cases per 100,000 women per year, which is lower than many African nations.
Speaking at one of the Integrated Child Health Days last year, Dr Annet Kisakye, said that, globally, the East African region carries the highest burden of cervical cancer.
According to research carried out by BMC Women's Health, Uganda has one of the highest incidence rates for CC in the world due to several barriers;
The most frequently reported barriers are an embarrassment, fear of the screening procedure or outcome.
Lack of access to cervical cancer screening services for those residing in hard to reach areas and limited resources for health infrastructure contributes to a higher prevalence rate.
Uganda introduced the HPV vaccine in November 2015, immunization was scheduled to be carried out in all the districts but coverage of the second dose has remained low years after its introduction.
To date, the Human Papillomavirus (HPV) prevalence rate among Ugandan women remains at a staggering 33.6%.
World Health Organisation reports that reductions of up to 90 per cent in HPV infections and genital warts in teenage girls and young women were registered in Europe and the United States as a result of using the vaccine.
This is hard to achieve in Uganda due to inadequate health infrastructure and lack of trained personnel.
In addition, poor follow-ups have hampered HPV interventions that work best with regular yearly screening intervals.
While the key goal for the Ministry of Health is to have 80% of the eligible 25-49 years screened, screening rates estimations are currently way below the target at 4.8 to 30%.
Screening for human papillomavirus (HPV) at most Uganda medical centres is erratic and can only be done when resources are availed by the government. In most cases, women are diagnosed with advanced disease.
The HPV vaccine
According to the Ministry of Health, the HPV vaccine does not contain any living or killed HPV virus. It is made from a single protein like the one the virus has on its outer coat.
When an individual has been vaccinated, the body produces antibodies, which it uses to fight the real virus when one is ever exposed to it.
The Ministry of Health is promoting a comprehensive approach towards the prevention of cancer of the cervix through immunisation with the HPV vaccine, screening, early treatment and sexual behaviour change.
The HPV vaccine targets HPV type 6, 11, 16 and 18 and it is best used to immunise girls before the onset of any sexual activity. Majority girls, who are at least 10 years of age, are less likely to be sexually exposed.
Therefore, immunisation reduces the cancer of the cervix by 60 to 70 per cent, girls can be immunised in schools or at health facilities currently providing routine immunisation services.
The Center for Disease for Control (CDC) recommends immunization of both boys and girls against the human papillomavirus –HPV.
CDC stresses that the vaccine protects a total of 9 types of HPV which are known to cause 99% of all cervical cancers.
The ideal time to vaccinate boys and girls is between ages 11 and 12, but it can be done as early as 9 years old.
Dr Noleb Mugisha while talking to the Daily Monitor at Mulago hospital recommended that regular screening to check for pre-cancerous lesions that could be treated early is a cost-effective preventive measure against cervical cancer.
The Ministry of Health recommends a two-dose schedule for the vaccine; the first and the second doses are given six months between each other. The vaccine is administered by injection in the upper arm.

In neighbouring Rwanda, for example, HPV vaccination achieved 93.23 per cent coverage in 2011, protecting up to 98,792 girls within the target age bracket of nine to 14 years.
The fight against cervical cancer in Uganda is not over yet, it is a tall order, a mountain climb derailed by the individual, social-cultural and structural factors such as;
Lack of knowledge
Poor knowledge of cervical cancer; the lack of awareness of the disease and availability of cervical cancer services is the major barrier.
Most women do not know about the cause of cervical cancer and many others have no idea on how and when to be screened.
Some women will not participate in the screening process because they find it is unnecessary in the absence of symptoms; they will only seek services at the onset of symptoms.
There have been negative perceptions of the HPV vaccine among Ugandans, with some shunning the immunisation exercise altogether.
In spite of the pre-vaccination sensitization; introduction of the HPV vaccine triggered several negative rumours that threatened acceptability among targeted adolescents and their parents.
Some girls refused vaccination because of unfounded rumours that they could become barren or face a greater risk of life-threatening childbirth complications,” reads in part.
This survey, the ‘Effect of School-based Human Papillomavirus (HPV) Vaccination on Adolescent Girls’ Knowledge and Acceptability of the HPV Vaccine was carried out in Ibanda District, Western Uganda and conducted by the Makerere University School of Medicine.
However, a release by the Ministry of Health debunks some of the myths associated with the HPV vaccine.
It indicates that HPV vaccine does not cause menstrual periods in babies, as alleged, because at that age, the hormones are inactive and neither does it cause hormonal imbalances because it is not a hormone.
The health ministry further explains that menstrual periods in girls are triggered by hormonal actions, oestrogen and progesterone.
The vaccine is given only to adolescent girls, not babies, and it does not have a contraceptive component or cause sterility as reported.
Vaccines Killings Africans
The ministry also indicates that it is also not true that the HPV vaccine was banned in most European countries and introduced in Africa to kill blacks as rumoured on social media.
The vaccine is still in use throughout the whole of Europe, the US and globally and it has been successful.
Embarrassment
The intimate nature of Pap smears deter most women from participating in the screening exercise, women decried lack of information and private spaces for self-collection of HPV swabs.
Most women also fear to become infected through non-disposable instruments and poor sanitary environments at health centres. There are rumours that the procedure might cause cancer or lead to enlargement of sexual parts and this send away their partners.
Stigma
Most women are afraid of receiving bad news when diagnosed with cancer saying that it will aggravate the condition.
Community members have a misconception about screening; a common preoccupation is that cervical cancer screening may reveal one’s HIV status.
Others are concerned that their partners will leave them if they are diagnosed with cancer.
Income and Family support
Women in relationships narrate that lack of their partner’s emotional and financial support is a barrier to cervical cancer screening. Households that earned more than 250,000 Uganda shillings per month have a higher intention to screen.
Traditional Healers
Health care workers report that women first seek advice from traditional practitioners because they believe cervical cancer is caused by witchcraft.

Limited access to health care
Women find it difficult to go for screening when health facilities are far away. In the BMC Women's Health Research, 33% of women who had never been screened attributed this to not having a nearby facility.
Lack of laboratory testing services and limited health infrastructure are also major barriers to cervical cancer screening.
Lack of Education
The study showed that women with higher education were significantly more likely to have been screened than their less-educated counterparts.
Community Sensitization
In one quantitative study by BMC Women's Health, women who attended community outreach services for cervical cancer screening were more likely to have engaged in screening services.
The Ministry of Healthy is broadening its call on the health sector and its various stakeholders to reach out to the affected population and not wait for people to approach them for services.
This multi-sector approach will engage health teams to conduct school and community-based sensitization, improve the disease prevention plan and beef up HPV immunization coverage.



Comments